

Understanding the Differences Between Vaginismus, Vulvodynia, and Vestibulodynia
Sophie Mason, PT, MSc PT, BSc (Hons.)
Pelvic Floor Physiotherapist

Key Takeaways
Vaginismus, vulvodynia, and vestibulodynia are distinct conditions that can all contribute to sexual pain and broader pelvic pain
The location and driver of pain can help differentiate these diagnoses
Treatment is most effective when it includes pelvic floor physiotherapy and a biopsychosocial approach
These conditions often overlap and require an individualized treatment plan
Why Understanding the Difference is Important
Pain with intimacy, touch, or penetration can often be grouped together under broad terms, but in reality, there can be numerous diagnoses contributing to pain in very small area.
Vaginismus, vulvodynia, and vestibulodynia each involve different structures and mechanisms. Without the appropriate distinction, treatment can miss the mark and lead to frustration, delayed progress, or persistent pelvic floor dysfunction.
Understanding both the anatomy and the root cause of symptoms allows for more targeted care, better outcomes and improved pelvic floor function.
Understanding the Anatomy
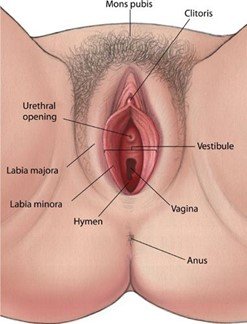
To understand these conditions, it helps to know the key structures involved:
Vulva: The external genital region, including the labia and clitoris
Vestibule: The sensitive area surrounding the vaginal opening
Vagina: The internal canal leading to the cervix
Pelvic floor muscles: A group of muscles that support the pelvic organs and contribute to continence and sexual function
The pelvic floor works closely with surrounding tissues and the nervous system. If one area becomes irritated or sensitive, it can influence the others and contribute to overlapping symptoms.
Defining the Conditions
Vaginismus
Vaginismus involves involuntary tightening of the pelvic floor muscles, especially around the vaginal opening. Frequently this is the body responding protectively, even in the absence of tissue injury.
Common features include:
Pain or difficulty with penetration
A sensation of “hitting a wall”
Anticipatory fear or guarding
Vulvodynia
Vulvodynia is chronic pelvic pain affecting the vulva, lasting at least three months without a clear identifiable cause. This condition can involve both tissue sensitivity and nervous system changes.
Symptoms may include:
Burning, stinging, or irritation
Constant or intermittent discomfort
Pain that is localized or more widespread
Vestibulodynia
Vestibulodynia is a subset of vulvodynia, with pain localized to the vestibule. This condition is often linked to increased sensitivity of the local nerve endings.
It is typically:
Triggered by touch or pressure
Sharp, burning, and highly localized
Associated with activities like insertion or wiping
Treatment: What Helps?
Vaginismus
Treatment focuses on reducing muscle guarding, improving control of the pelvic muscles and reducing the reflexive protective muscle response:
Pelvic floor relaxation and downtraining
Breathing and nervous system regulation
Gradual desensitization and exposure (e.g., dilators)
Education and reassurance
Vulvodynia + Vestibulodynia
Treatment may include:
Nervous system desensitization
Targeted tissue desensitization + graded exposure to touch
Skin and tissue care
Pain education
Addressing contributing factors (hormonal, musculoskeletal, inflammatory)
Addressing secondary pelvic floor tension
Medical or topical support when appropriate
Why a Biopsychosocial Approach Matters
These conditions are not purely physical, and they are not “just in your head”. Sometimes, it’s important to recognize that the pain is not in your head, but the solution is not entirely in your body either.
A biopsychosocial approach considers:
Biological factors: tissue sensitivity, inflammation, muscle tension
Psychological factors: fear, anxiety, past experiences, pain beliefs
Social factors: relationships, communication, and support systems
Pain with intimacy can carry emotional weight, and repeated painful experiences can increase nervous system sensitivity and protective responses in the pelvic floor.
This is why pelvic physiotherapy is most effective when it supports both the body and the nervous system as part of comprehensive rehabilitation plan.
At Proactive Pelvic Health Centre, care is individualized, evidence-based, and compassionate—because lasting progress requires addressing the full picture.
Final Thoughts
If you are experiencing pelvic pain or sexual pain, understanding the source of your symptoms is a powerful first step.
With the right diagnosis and support from a qualified pelvic floor physiotherapist, meaningful improvement is absolutely possible.
References
International Society for the Study of Women's Sexual Health (2019). Consensus terminology and classification of persistent vulvar pain and vulvodynia.
American College of Obstetricians and Gynecologists (2020). Persistent Vulvar Pain (Committee Opinion No. 673).
International Continence Society (2010). Terminology of pelvic floor muscle function and dysfunction.